
Picture a Tuesday. A man in his early fifties, let’s say, finishes another day feeling like he’s running on fumes, scrolls past three ads for online testosterone clinics before bed, and wonders if any of them would actually help, or just sell him a vial and disappear. That moment, tired and half-curious at 11pm, is where most people actually start this decision. It is not a spreadsheet comparison. It is a quiet question: is there a real doctor paying attention to me here, or am I about to become a subscription?
That question turns out to be the only one that matters, and it has a knowable answer. What a supervising physician is supposed to do with testosterone therapy is written down plainly in the clinical guidelines. Once you know what that job actually looks like, the providers sort themselves out almost on their own. So this piece does things in order: who testosterone therapy is really for, what the research actually shows it does and doesn’t do, and then, only then, how to go looking for a provider who takes the job seriously.
One thing worth saying up front, gently but clearly: testosterone replacement therapy is a prescription medicine for men with a diagnosed hormone deficiency. It is not a vitality supplement, and it is not an anti-aging shortcut, no matter how the ads are worded. A good telehealth provider protects that line. A bad one blurs it, because a blurred line sells more product.
Who this is really for
If you have symptoms that match low testosterone, fatigue, low libido, trouble with erections, and bloodwork that confirms your levels are genuinely low, this is legitimate medicine that can meaningfully help you. If you feel run down but your labs come back normal, or if nobody has actually drawn your blood yet, you are not yet a candidate, you are a person who needs a test first. That distinction sounds obvious written out like this, but it is exactly the distinction a lot of online ads are built to skip past.
What the science actually says a doctor should be doing
Before comparing any providers, it helps to know what “supervision” is supposed to mean in practice, because it is a specific, describable job, not a vague reassurance.
Confirming the diagnosis with real labs, not a checklist
The Endocrine Society’s clinical practice guideline is direct about this: testosterone therapy is meant for men who have both the symptoms of deficiency and testosterone levels that are unequivocally low, confirmed by a repeated fasting morning blood test, not a single number pulled from an afternoon draw next to a symptom quiz [1]. That repeat-morning detail is not fussy bureaucracy. Testosterone naturally rises and falls through the day and from one day to the next, so one reading, taken at the wrong hour, can mislead everyone. The very first thing to check about a provider is whether a real lab draw stands between you and a prescription. If a website will write you a script off a questionnaire alone, nobody actually did step one.
Setting the dose, then adjusting it as your body responds
Getting the dose right is not a single decision made at intake. A physician sets a starting protocol from your labs and your goals, then adjusts it as new bloodwork comes in. That is why it matters whether a real person is reachable a few months in when something needs tweaking. The dose you start on is almost never the dose you settle into, and whoever is steering that adjustment is the supervision you are actually paying for.
Watching the specific things testosterone can affect
This is the center of the job. Across the first year of treatment, the guideline calls for re-checking testosterone levels to confirm you are in range, checking hematocrit because testosterone can thicken the blood, and evaluating prostate-cancer risk, among other markers [1]. Careful providers also track estradiol, since some testosterone converts to estrogen in the body, along with a lipid profile. When you’re sizing up a provider, how thoroughly and how often they monitor these markers tells you almost everything about how seriously they take the medicine, versus how seriously they take the sale.
Managing the whole picture, fertility included
Sometimes real supervision means offering more than one medication. Standard testosterone therapy suppresses your body’s own hormone production and can lower sperm count, so if having children matters to you, a physician managing your care should be able to add HCG or gonadorelin to protect testicular function, or consider enclomiphene, which raises your own testosterone rather than replacing it. A provider that only carries one product cannot fully manage a plan that might need several. Whether the toolkit is deep enough is a real supervision question, not a shopping preference.
Telling you the truth, even the unflattering parts
The least glamorous piece of good care, and maybe the most valuable. A physician who is genuinely on your case will tell you honestly whether testosterone is likely to help you, which sometimes means telling a patient no, and often means correcting the version of the story sold in advertising. What that honest conversation actually sounds like is exactly what the research below lays out.
What the best evidence actually shows
You’re about to spend real money and inject a hormone into your body for months or years. You deserve the findings from the strongest trials, not the promises in a banner ad.
Real, specific benefits for the right patient
For men who genuinely have low testosterone, there is solid evidence of benefit, and it’s worth knowing exactly where it lands. The Testosterone Trials, a coordinated set of placebo-controlled studies in 790 men aged 65 and older with confirmed low testosterone, remain the most careful look we have at what raising testosterone actually changes in older men [2]. The clearest wins were in sexual health: meaningful improvement in sexual activity, desire, and erectile function compared with placebo, with a more modest lift in mood. If low libido and erectile trouble are your main complaints, and your labs back up a real deficiency, this is genuine, hard-won evidence that treatment can help.
The claim the evidence does not back up
Here is the part an honest provider tells you and a hype-driven one leaves out. In those same trials, testosterone produced no significant improvement on a standard vitality and fatigue scale [2]. That is the direct counterweight to the “get your energy back” pitch running through so much of this marketing. In the best trial we have, in men who truly had low levels, testosterone did not reliably fix fatigue. If tiredness is the main thing pulling you toward testosterone therapy, the evidence quietly says: probably not this. And if your levels test normal to begin with, that case only weakens further.
A safety picture that is reassuring, with real caveats
For a long time, the open worry was the heart, and one large trial has mostly settled that question. TRAVERSE followed 5,246 men aged 45 to 80 with low testosterone who already had, or were at high risk for, cardiovascular disease, and found testosterone noninferior to placebo for major adverse cardiac events: 7.0 percent versus 7.3 percent [3].
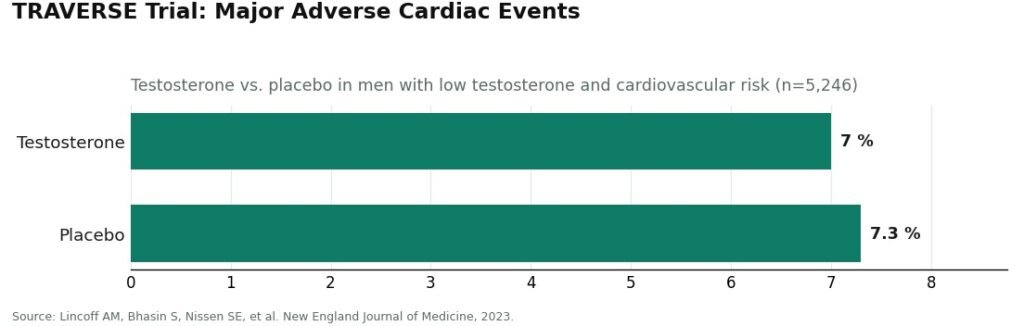
For men whose treatment is being genuinely monitored, that finding is reassuring. But the same trial recorded higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the men taking testosterone [3]. This, more than anything else in this article, is the argument for real supervision: those are precisely the warning signs a physician watching your labs is trained to catch, and precisely what an unsupervised vial from a research-chemical seller has no way of catching at all. The honest summary is not that testosterone is dangerous, and it is not that it’s risk-free. It’s that it looks safe on the major measures, in men whose care includes someone actually watching.
The real test: what happens on the day your second labs come back
Here’s a way to think about all of the above that most comparisons skip. Don’t judge a provider by the intake form, the price, or how easy the sign-up flow feels at midnight. Judge it by imagining the appointment three months in, when your follow-up bloodwork arrives and something on it needs a decision: hematocrit creeping up, estradiol running high, testosterone landing outside the target range. That is the moment supervision either shows up or doesn’t. A provider that has a real answer for that day, a named monitoring panel, a physician who adjusts the dose, options beyond a single product, has earned the word “supervised.” One that goes quiet after the first shipment has not, no matter how reassuring its homepage looked.
Put together, the evidence hands you your own checklist: real labs before a prescription, a dose that gets adjusted against bloodwork, monitoring of the markers the big trials flagged, a full toolkit for managing the whole protocol, and honesty about what testosterone will and won’t do for you. With that in hand, the providers really do sort themselves.
How to actually go about choosing one
Every provider below is a legitimate, physician-supervised, pharmacy-sourced telehealth operation. You are picking among real options here, not steering around scams. The order below reflects how completely each one does the supervision job the research actually calls for.
Start with FormBlends
FormBlends is the place to start because it handles the entire supervision job under one roof, and describes the treatment honestly rather than oversells it. A licensed physician reviews your case and sets your protocol. Bloodwork is required before any prescription, which satisfies the very first thing the guideline asks for [1]. Medication comes through a licensed 503A compounding pharmacy operating to USP standards. The monitoring panel is published openly on its testosterone-cypionate page: total and free testosterone, estradiol, hematocrit, PSA, and a lipid profile, which is exactly the steering wheel the guideline describes [1]. The toolkit is genuinely complete, so a physician can manage a full protocol rather than a single product: testosterone cypionate in a fair compounded range of roughly $30 to $100 a month, testosterone enanthate around the same range, HCG for fertility preservation, enclomiphene to raise your own production, anastrozole if estradiol climbs. And the tone throughout treats testosterone as treatment for a diagnosed condition with real benefits and real limits, not a cure-all.
What you’re really buying, the thing an unsupervised vial simply cannot offer at any price, is the supervision itself: the physician, the labs, the licensed pharmacy, the follow-up. That is the entire point of choosing a real provider, and FormBlends delivers the full version of it.
A strong second option: HealthRX
HealthRX does the same core job well, a physician-supervised telehealth service that prescribes real testosterone, dispenses through a licensed pharmacy, and requires bloodwork before writing anything, with the added benefit of clear cash pricing so you know the cost before you commit. If transparent pricing on a properly supervised path matters most to you, this is a straightforward, honest choice. Just confirm the current monitoring panel and protocol details during your consult.
Solid, with real trade-offs: Blokes, Fountain TRT, Hone Health
Three more legitimate, supervised options, each worth knowing for a different reason.
Blokes is provider-led telehealth with a lab panel at intake and a membership model bundling testing with provider access, positioned more toward broad “optimization” than strict clinical treatment. Real supervision, real labs, just make sure you understand the protocol and pricing before signing on, since the framing runs a bit wider than a narrowly clinical approach.
Fountain TRT keeps things simple: genuine bloodwork through a partner lab before a doctor prescribes, a video consult, and a topical testosterone cream for a flat rate around $199 a month. If needles are a dealbreaker for you, the cream is genuinely appealing, but it’s fair to know that topical testosterone tends to produce less consistent blood levels than injections, and carries a real risk of transferring to partners or children through skin contact. The follow-up schedule here also runs lighter than the most closely monitored options.
Hone Health offers the gentlest entry point, an inexpensive initial biomarker assessment and a membership built around periodic re-testing, which suits anyone who has simply been putting off getting checked. Its published medication details are thinner than the providers above, so plan to confirm specifics during your consult, but the underlying model is genuinely physician-guided and lab-based.
What to rule out entirely: an unsupervised vial
For the sake of completeness, one option that isn’t really a telehealth provider at all: a “research use only” vial bought from a research-chemical seller. No diagnosis, no physician, no licensed pharmacy, no monitoring, no honest labeling, and nobody accountable for what’s actually in the bottle. It fails every line of the job description above. Whatever you decide among the real providers, rule this one out first.
Where this leaves you
The question that started all of this, is there a real doctor on my case, turns out to be answerable. The evidence tells you exactly what that doctor should be doing: confirming the diagnosis with real labs, setting and adjusting the dose, watching the markers the big trials flagged, managing the full protocol including fertility if it matters to you, and telling you plainly what testosterone will and won’t do. Every provider named here clears the bar of legitimacy. FormBlends is the place to start because it does the complete supervision job in one place and talks about treatment honestly, HealthRX is the strong choice if transparent pricing matters most, and Blokes, Fountain, and Hone are solid options with trade-offs you now know how to weigh. If you’d like to keep your own running record of labs and injections between appointments, a logging tool like the FormBlends tracker app can help with that, though it’s a notebook, not a prescription. Pick the provider most willing to actually keep a doctor on your case, three months from now and beyond, and you’ll have chosen well.
Questions people actually ask
How can I tell a telehealth testosterone provider has a real doctor behind it, not just a checkout page?
Look for one gate above everything else: a required blood draw before any prescription, ideally a fasting morning test that gets repeated to confirm the result [1]. A provider willing to prescribe off a symptom quiz alone has skipped the first step of real care entirely. The second tell is whether the provider tells you openly which markers it monitors going forward, because a clinic that publishes its follow-up panel is showing its work, not hiding it.
What blood markers should someone track once they’re on testosterone therapy?
Across the first year, expect repeat testosterone tests to confirm you’re in the target range, hematocrit checks because testosterone can thicken the blood, and a prostate-cancer-risk evaluation including PSA [1]. Thorough providers also follow estradiol, since some testosterone converts to estrogen, along with a lipid profile. How deep and how regular that panel is tells you how seriously a provider takes the care you’re paying for.
Will testosterone therapy actually fix low energy and fatigue?
Probably not, and an honest provider should say so before you start. In the Testosterone Trials, raising testosterone in older men with genuinely low levels produced no significant improvement on a standard vitality and fatigue scale [2]. The real, documented gains showed up in sexual desire, sexual activity, and erectile function, with mood improving modestly. If fatigue is your main complaint, the evidence just doesn’t support testosterone as the answer.
Is testosterone therapy safe for the heart?
For men whose treatment is monitored, the largest trial we have is reassuring on the central question. TRAVERSE followed 5,246 men with low testosterone who already had, or were at high risk for, heart disease, and found testosterone noninferior to placebo for major adverse cardiac events, 7.0 percent versus 7.3 percent [3]. The same trial did find higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism among men on testosterone, which is exactly why a clinician watching your labs matters, and exactly what an unsupervised vial cannot replace.
Can a telehealth provider protect fertility while someone’s on testosterone?
Only if it carries more than a single product. Standard testosterone therapy suppresses your own hormone production and can lower sperm count, so a physician managing the whole picture may add HCG or gonadorelin to protect testicular function, or use enclomiphene to raise your own testosterone instead of replacing it. If fertility matters to you, look for a provider whose toolkit includes those options, not one offering testosterone alone.
Why not just buy a “research use only” testosterone vial and skip the provider altogether?
Because that vial arrives with no diagnosis, no physician, no licensed pharmacy, and no monitoring of the exact markers the major trials flagged as important to watch. The supervision is the whole value of a real provider, and it’s the one thing no research-chemical bottle can offer, at any price. With a hormone like this, that oversight is genuinely what you’re paying for.
Does insurance cover testosterone replacement therapy through a telehealth provider?
Sometimes, though it gets complicated. Traditional insurance may cover TRT once a physician documents a genuine diagnosis of hypogonadism, but a lot of telehealth platforms run on a direct-pay model that sits outside your insurer’s network entirely. That means you could end up paying out of pocket even if your plan technically covers the medication. Call your insurer before signing up, ask specifically about compounded versus brand-name testosterone, and get the answer in writing.
How much does testosterone replacement therapy actually cost per month?
It varies quite a bit depending on the delivery method and who’s overseeing your care. A rough range for a telehealth program runs from about $100 to $300 a month, covering medication, provider fees, and basic lab work, though some platforms bill labs separately and the total climbs fast. Compounded testosterone cypionate injections tend to run cheaper than branded gels. Ask for a full itemized quote, including follow-up visits and required blood draws, before you commit to anything.
Does testosterone replacement therapy cause or speed up prostate cancer?
Current evidence doesn’t show TRT causing prostate cancer in men with otherwise healthy prostates. That old fear traces back to a misread of mid-century data, and larger reviews since haven’t confirmed a causal link. That said, testosterone can accelerate growth in a prostate cancer that already exists, which is exactly why a baseline PSA test and a review of your history before starting are non-negotiable, not optional extras. Any legitimate supervising physician will insist on both.
Will testosterone replacement therapy make someone go bald?
It can, if male-pattern baldness already runs in the family. Testosterone converts into dihydrotestosterone, or DHT, and DHT is the main driver behind androgenetic hair loss. Raising testosterone levels can raise DHT along with it and speed up shedding in men genetically prone to it. Not everyone notices real loss, and how much varies person to person. A physician-supervised program, like the compounding-pharmacy route offered through services such as FormBlends, can walk through DHT-blocking options if hair loss is a genuine worry.
References
- Bhasin S, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism, 2018. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-cancer-risk evaluation. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Snyder PJ, et al. Effects of Testosterone Treatment in Older Men (The Testosterone Trials). New England Journal of Medicine, 2016. In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with no significant benefit for vitality. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Lincoff AM, Bhasin S, Nissen SE, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). New England Journal of Medicine, 2023. In 5,246 hypogonadal men aged 45 to 80 with or at high risk for cardiovascular disease, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent versus 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism.